This Channel 4 programme by Rogan Productions and broadcast on May 20, included contributions from NALC Vice-President Trevor Hutson and wife Sally – they can be seen below
Catch up on All 4 if you missed it.
This Channel 4 programme by Rogan Productions and broadcast on May 20, included contributions from NALC Vice-President Trevor Hutson and wife Sally – they can be seen below
Catch up on All 4 if you missed it.
NALC is contributing to webinars organised by Severn Healthcare. They will use the Zoom platform. Many laryngectomees have been using Zoom during the lock-down to communicate with family and friends. Others may be unfamiliar with its use so some assistance is given here.
If you apply to join the meeting you will receive a link in an email. To join the meeting click on the link at the appropriate time. Beforehand you may want to make sure your device is ready and learn a bit about your options during the meeting.
Zoom can be accessed using a smartphone or tablet using an app downloaded from the relevant store. Alternatively with a laptop a browser such as Chrome or Edge can be used The link below can be used to test the laptop setup and internet connection to ensure Zoom will work.
A user guide (pdf) is here
HowtoParticipateInAZoomMeeting
The NCRI produced a powerpoint presentation about using Zoom
UPDATE 24/6/20
As was correctly reported last week, shielding will end on July 31st. Further announcements about changes, such as reducing social distancing to 1 metre in some situations, are coming thick and fast. I suspect many of the vulnerable and extremely vulnerable will be making decisions to keep safe, just as they did before the lock-down. The situation, for many, may be getting a bit confused and further guidance is needed in good time.
This article raises some valid concerns.
UPDATE 18/6/20
The Health Service Journal has reported shielding is likely to continue until July 31st.
If you are currently shielding and are not getting the support needed then this may help
UPDATE 25/5/20
Public Health England have advised us that laryngectomees are not going to be added to the extremely vulnerable group. However there is a route an individual can take and that is to seek help from their GP or hospital clinician who have the power to add the patient to the group. In my experience hospital clinicians have provided better support to our community.
The current period for which this group have been asked to isolate completely at home extends to the end of June. There remains the possibility they may be advised to continue to do this for even longer, and I assume would continue to get the extra support with the delivery of shopping and medications.
UPDATE 30/4//2020
The CLT have been advised “the Chief Medical Officer’s office have now confirmed that their panel will consider this issue”. We await further news of the timing.
UPDATE 26/4/2020
NALC joined many clinicians groups such as RCSLT, BAHNO and ENT UK in sending a joint letter to Public Health England last week asking that laryngectomees be added to the list. We await a response and in the meantime contacting a GP for support (see below) in getting on the list is the best option.
Important information came from a response to the Cancer Larynegctomy Trust:
From: CANCERPOLICY, England (NHS ENGLAND & NHS IMPROVEMENT – X24) <england.cancerpolicy@nhs.net>
Sent: 09 April 2020 10:50
Subject: RE: Laryngectomy
Yes, someone who has had a laryngectomy is likely to be considered extremely vulnerable as the upper airway cannot be protected as well as usual. Patients should discuss directly with their cancer care team and GP, who will have discretion to add them to the vulnerable list. In the meantime, if they are concerned about their risk of infection they should follow the shielding guidance.
With best wishes,
Kasia
Kasia Olszewska
Parliamentary and Briefings Officer
NHS Cancer Programme
NHS England and NHS Improvement
NALC has had several communications from clubs about the risk status of laryngectomees and the absence of a categorical statement of our inclusion in the list of at risk groups. NALC is joining with clinician groups like the BLA to pass a strong message to NHS England that we should be specifically included in the lists. This will help in many ways, not least in convincing employers that it is not safe for laryngectomees to turn up to work as normal and accommodations must be made.
It is possible for patients and/or carers to request to be added to the “extremely vulnerable” group. We are aware of laryngectomees who have successfully used the link below, but others have been rejected. The link is:
www.gov.uk/coronavirus-extremely-vulnerable
On the BBC News website it was reported on April 7th:
NHS Digital, which compiled the list of the vulnerable, said it had identified about 900,000 patients who should have already received an official letter or text.
However, it said GPs and hospital doctors were now adding a further 600,000 patients.
It also advised people to register themselves on the website (see above) if they needed extra help and support.
The Department for Environment, Food and Rural Affairs (Defra) and the Royal College of General Practitioners have also advised those who feel they had been missed off the list to contact their GPs.
Covid 19 is a new virus. It is impossible to have information about how exactly laryngectomees may be at risk. Hopefully NHS England will choose to take a safety-first approach in meeting our needs and add us to the vulnerable group on request.
UPDATE May 17
BLA, ENTUK and RCSLT have produced new guidelines as services slowly return to normal. Of particular note is the statement:
“As voice prosthesis care is considered an AGP, full PPE will be required with post procedure cleaning / decontamination procedures in line with PHE guidance and local infection prevention control.”
(AGP – aerosol generating procedure)
Patients need to be aware of the impact of the coronavirus pandemic on the way their hospital will deliver care. On March 25th the British Association of Head and Neck Oncologists published this:
BAHNO recognises that the management of many patients with cancer will have to be modified during the current COVID-19 crisis. One particular group that may cause management dilemmas are those with voice prostheses.
Reinsertion of tracheooesophageal puncture (TEP) voice prostheses
Cyrus Kerawala
The National Tracheostomy Safety Project (NTSP_UK) has published some advice for laryngectomees and tracheostomees
NTSP Advice for patients with a tracheostomy in the Coronavirus pandemic
ENT UK Patient FAQ COVID-19 March 30th 2020
Background
This document has been prepared in response to the numerous patient and professional queries received through social media and direct phone contact. It is intended to support the ENT UK documents produced and is aimed at the layperson. It is presented in a Q&A format.
Questions and answers
Q: I have a new cough but no other symptoms; should I isolate from the rest of my family?
A: Yes. As per present guidelines, you should self-isolate from rest of your family who should also be isolating at home as per present UK government instructions.
Q: I have lost my sense of smell but otherwise feel fine. Do I have COVID-19 and should I self-isolate from family?
A: It is reasonable to assume that the new loss sense of smell (anosmia) is COVID-19-related and you should follow guidelines for self-isolation from the rest of your family group.
Q: I have lost my sense of smell. When is it likely to come back?
A: Reports from other countries such as Italy seems to suggest that COVID-19-related loss to your sense of smell should return within 7-14 days. It is of course possible that the loss is due to other causes such as sinusitis, or other viral infections, but those also have good rates of recovery.
Q: I normally take nasal steroid sprays and have now lost my sense of smell. Can I continue taking them?
A: Yes, you can. There is some evidence that oral steroids can make the severity of COVID19 infections worse, so although oral steroids have previously been used in people with new symptoms of anosmia, we would not recommend these at the present time.
Q: I am a key worker without direct patient contact, but live with others with pre-existing conditions. Can I still go to work?
A: Yes, you can. As long as neither you nor any member of the household is experiencing any symptoms, you may go to work and observe all social distancing rules on your journey.
Q: If I think I have had COVID-19, can I stop self-isolating from family after 7 days, even if I don’t feel back to normal?
A: Yes, you can. However, if you have deteriorating symptoms, particularly increased shortness of breath, and you are struggling to breathe, you should seek medical advice via 111 or, if very unwell, presenting to hospital.
Q: I am meant to have an ENT operation. Will I still be able to have it?
A: Not at the present time. Most, if not all, elective operations have ceased for the time being so unless you are due to have a cancer-related operation, it is very likely that your operation will be postponed to a later date.
Q: I am meant to have an ENT outpatient appointment. Will this still go ahead?
A: Not at the present time. You may still be contacted by phone to have a virtual/phone consultation, but it is very unlikely that you will be attending clinic. If your appointment is cancelled, it will be rebooked for a later time.
Acknowledgements Thank you to Prof Carl Philpott and Prof Claire Hopkins, as well as the ENT UK executive committee for their input and guidance. References 1. ENT UK advice for patients with new-onset anosmia during COVID 2. Initial guidance for head and neck cancer management during Covid-19 Nara Orban Consultant ENT Surgeon Ass Hon Sec, ENT UK.
ENT UK at The Royal College of Surgeons of England 35-43 Lincoln’s Inn Fields London WC2A 3PE Tel: 020 7404 8373 | Email: entuk@entuk.org | Web: www.entuk.org
NALC has sought assistance from its medical advisors to produce advice for our community in the difficult situation facing us, with a possible coronavirus epidemic.
SPECIFIC ADVICE
We want to highlight two essential ways the risk of contracting the virus can be reduced. Laryngectomees differ from others with the only route into the lungs being through the stoma.
GENERAL ADVICE
IF YOU FEEL UNWELL – updated regularly
If you have the symptoms below
Follow the latest Government advice
OTHER
The American physician, and laryngectomee, Dr Itzhak Brook has written about coronavirus on his blog
Northampton General becomes first hospital to treat head and neck cancer using artificial intelligence
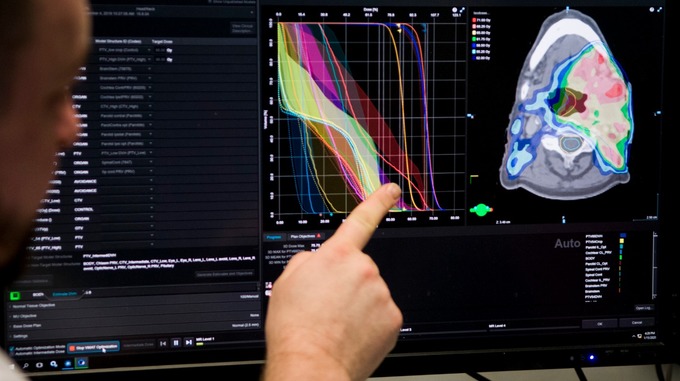
Dr Craig Knighton looks at a treatment plan in progress Credit: Northampton General Hospital
Radiotherapy patients at Northampton General Hospital are among the first in the UK to be benefiting from the use of artificial intelligence. It’s being used to determine the best treatment for head and neck cancer, a particularly complex area to treat due to the proximity of radio-sensitive organs like the face, spine and brainstem.
The revolutionary software, called ‘RapidPlan’, learns from the last 100 treatments at Northampton General to generate an individualised plan for new patients.
Not only does this new way of working provide patients with the best possible treatment for their needs, but with minimal human interaction, it saves time. Before this, clinicians and medical physics staff would have spent time analysing scans to decide on a treatment that satisfies the many rules for a plan.
“Using this new technology gives our clinicians instant access to the information stored in previous treatment plans, to generate high quality treatment plans in a reduced timeframe. This will allow shorter waiting times and increased numbers of patients treated.”
– DR CRAIG KNIGHTON, CLINICAL DIRECTOR OF ONCOLOGY AND HAEMATOLOGY
The hospital hopes the new system, made by the company Varian, will help create more consistency across departments. Staff are also looking to create a supermodel for radiotherapy treatment across the country.
(From an ITV report)
How do head and neck patients fare in comparison with others?
Head and neck cancer is considered a “rare” cancer. Because the patient numbers are low compared to say breast or prostate cancer it can be difficult to gather meaningful information because sample sizes in surveys are too low.
The National Cancer Patient Experience Survey has been running for some years and the latest included returns from almost 2000 head and neck patients. Even so, results for our patients from individual trusts are problematic due to the small sample size for each and little information is available. Statistically significant results are only presented for the whole country.
Care is needed in comparing the experiences of patients having different cancer types. Differences in the care pathway, including preferred treatment modalities, will lead to differences in the response to particular questions in the survey. However some interesting differences are evident in the results. Looking back at previous surveys as well, the same differences have been seen in previous years.
When asked about the time between them noticing something suspicious to consulting a GP, 8% of head and neck patients reported a delay greater than 6 months. 3% of breast cancer patients gave the same answer.
A similar divide was seen after the visit to the GP. For 18% of head and neck patients it took 3 or more GP visits to get a referral to a hospital but just 3% of breast cancer patients needed this many.
When asked if they were given written information about their cancer, in a form that was easy to understand, 50% of head and neck patients responded positively. The corresponding figures for prostate and breast cancer were 74% and 70%.
These differences do not necessarily reflect failings in treatment and care; they will also result from the varying challenges of dealing with cancer at different tumour sites.
For patient support and advocacy groups, the results of the survey are valuable in assessing priorities and from the examples above raising awareness about head and neck cancer stands out.
The NCPES provides valuable information and would reward deeper analysis than presented here. I do hope the NHS will continue to fund this work and it does not go the same way as the head and neck audit (DAHNO) and vanish.
The linked article below is a comprehensive and useful guide raising awareness of head and neck cancer symptoms. Though the focus is on laryngeal and pharyngeal cancers, there are links to information about other head and neck cancers. Though the scenario is the USA, it is equally relevant for the UK.
There is ample evidence of the serious consequences of delaying treatment. The risks are currently enhanced by a reluctance to seek medical assistance, especially by men, and the current pressures on the NHS, leading to a failure to meet targets for treatment deadlines.
Ensuring information in this article is spread as widely as possible has to be a priority if lives are to be saved.
Functional problems after treatment for head and neck cancer are the bane of so many patients lives. Speech is inevitably an issue, especially for laryngectomees, but swallowing problems cause so much distress as well.
I recently met a laryngectomee who has never found an alternative voice, aside from phone apps. Now, six years down the line, he has additionally begun to experience problems with swallowing.
Researchers at the University of Alberta in Canada have developed a device that can extend the swallowing function from liquids only to a more normal diet.
It is early days and the research only involved a small number of patients but hopefully such strategies will enable future patients to have a better quality of life after treatment.
There are plenty of sources of information describing best practice in the treatment of head and neck patients. They range from the 2015 document “Achieving World Class Outcomes”, many NICE guidelines and quality statements and the 2012 NHS document “Nothing About Me Without Me” .
A recent article in the Nursing Times describes the head and neck pathway at UHNM, in Stoke.
There are many impressive features of the care they provide and I especially like a couple.
The team provide their patients with peer support, stratified into 3 streams head and neck, laryngectomee and thyroid.
Secondly there is an emphasis on patients being involved in decision-making about their care. Choice between alternative treatment options is highlighted in NICE guidelines and the patient view should figure highly in any such discussions.